
Somewhere along the way, “peptides vs steroids” became a normal thing to type into a search bar. It sounds like a fair fight between two similar things. It isn’t. One of these words names a federally controlled drug class with a well-documented trail of heart and hormone damage. The other names a category so wide it holds both a heavily studied diabetes medication and an unproven powder someone mixed in a warehouse. Asking which one wins is a bit like asking whether you’d rather have “a car” or “transportation.” The question doesn’t hold together, and people get hurt trying to answer it anyway.
So this isn’t a face-off. It’s a sorting exercise. The goal is simple: by the end, tell these two categories apart on sight, because that habit alone protects people more than any single fact on this page.
Steroids, plainly
Anabolic-androgenic steroids (AAS) are synthetic cousins of testosterone. They latch onto androgen receptors across the body, which is exactly why they build muscle and also why they touch so many other systems at once. In the United States, they sit as Schedule III controlled substances, the same legal tier as testosterone itself and ketamine, a classification meant to reflect a real, intermediate risk of misuse [1].
That legal status matters before anything else does. A physician can legitimately prescribe testosterone for a diagnosed condition. What that is not is the high-dose, muscle-building use people picture when they hear “steroids,” and getting AAS without a prescription is a federal offense, full stop. No “research use only” label changes that.
The harm data deserves a plain read, not a softened one. A 2026 systematic review and meta-analysis in the International Journal of Cardiology, pooling 35 studies and roughly 2,000 men, found steroid users had lower left ventricular ejection fraction, worse global longitudinal strain, thicker heart walls, and greater left ventricular mass than non-using athletes [2]. In everyday terms: hearts working less efficiently, inside walls that had grown thicker than they should.
The hormonal side surprises people, because it runs backward from what they expect. Add enough outside androgens and the body stops making its own. A 2023 scoping review in Endocrine Connections on steroid-induced hypogonadism found recovery of natural testosterone and fertility afterward is genuinely uneven, tied to age and how heavily someone used, with testicular size and sperm production sometimes taking years to return, if they return fully at all [3]. Someone chasing a stronger body can end up with a weaker hormonal one instead.
None of this erases the fact that steroids do build muscle. That was never in question. What’s in question is whether that effect is worth a documented, serious harm profile, taken on entirely without legal protections or medical oversight.
Peptides, plainly
This is where sorting gets interesting, because “peptide” isn’t one thing at all. A peptide is simply a short chain of amino acids, a definition loose enough to catch molecules with almost nothing else in common.
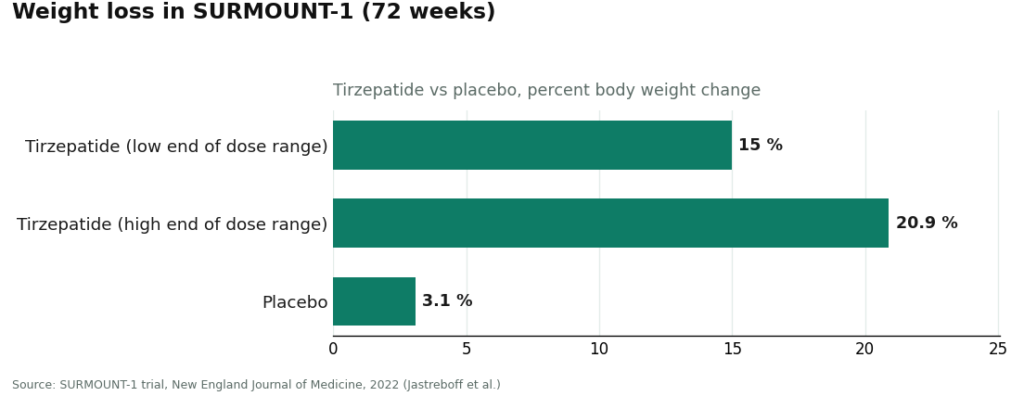
On one end sit some of the most carefully tested medicines in current use. Semaglutide and tirzepatide, the GLP-1 drugs everyone’s discussing, are peptides by structure. StatPearls describes this class as incretin-based agents that raise insulin secretion, lower glucagon, slow gastric emptying, and increase satiety [4]. The trial evidence behind them is substantial. In SURMOUNT-1, published in the New England Journal of Medicine, participants on tirzepatide lost between 15.0% and 20.9% of body weight across doses over 72 weeks, versus 3.1% on placebo [5]. That’s a peptide with a real, peer-reviewed evidence base behind it.
On the other end sit the research-status peptides, names like BPC-157 and TB-500, sold for healing and recovery with human evidence that ranges from early to nearly absent. The marketing tends to run years ahead of the science. These typically arrive online labeled “for research use only,” with no clinician and no pharmacy anywhere between manufacture and mailbox.
If one idea sticks from this page, let it be this: the proven end of the peptide world and the unproven end are not the same product wearing different labels. Treating them as interchangeable is either careless or a sales tactic.
Why people reach for each
People reach for anabolic steroids for one main reason: to change how the body looks and performs, quickly. That pull is real, and there’s no need to shame it here. The trouble is that the fastest route is also the controlled, high-harm, no-oversight one.
People reach for peptides for messier reasons. Some want the same body-composition change and have heard the GLP-1 drugs deliver it through a completely different mechanism. Others are drawn to recovery, sleep, or longevity claims tied to the research-status compounds, often without realizing how thin that evidence still is. The two groups overlap in what they want and diverge sharply in what the evidence actually backs up.
Set the two side by side and the contrast makes its own argument: GLP-1 peptides with a published trial record and a legal path through a clinician [4][5], against illicit steroids with documented cardiac and hormonal costs [2][3].
So which is “safer”?
Honestly, it depends entirely on which specific thing is being asked about, and that’s the whole reason the blanket comparison fails.
An FDA-approved peptide taken under medical supervision, with a clinician checking history and contraindications, is not the same proposition as an unverified research powder, which is again not the same as an illicit steroid. These aren’t three points on one dial. The one comparison that actually holds up is between unsupervised illicit steroid use and a specific peptide obtained through medical care, and in that comparison the supervised route is plainly the more responsible choice. Notice the word doing the work there: supervised. An unsupervised compound of either kind clears no real safety bar.
What a supervised path looks like
If someone decides to pursue the legal, supervised side of this, the structure that protects them isn’t complicated. A licensed clinician reviews their history. A prescription gets written where it’s appropriate. A licensed pharmacy fills it. Someone stays medically accountable afterward. That’s the layer a gray-market sale can never offer, since the entire point of a “research use only” listing is that no clinician and no pharmacy are involved.
Supervised telehealth providers built around that structure, FormBlends among them, occupy a different category entirely from a powder shipped with a disclaimer, and further still from sourcing a controlled steroid illicitly. Naming it here is meant as an example of what supervision looks like, not a sales pitch. The clinician who can tell someone a compound is wrong for them, before it’s ever taken, is worth more than any product claim on a label.
One caveat belongs here plainly. Many compounds in this supervised space are compounded medications, and compounded medications are not FDA-approved finished products, nor evaluated by the FDA for safety, effectiveness, or quality. Supervision adds oversight around the process. It doesn’t make a compounded preparation equivalent to an approved brand-name drug. And the research-status peptides still carry limited human evidence no matter who hands them over. A good clinician says that plainly. So should any honest explainer.
The short version
Anabolic steroids are a controlled substance with documented, serious harms to the heart and to natural hormone production [1][2][3]. Peptides are a much wider category, one where a few standouts, the GLP-1 drugs especially, are exceptionally well studied [4][5], while many others are barely studied at all. They don’t belong in the same head-to-head, as if they were two brands competing for the same shelf space. Anyone weighing these options is better served by a conversation with a licensed clinician than by a checkout page or an illicit source.
Common questions
Are peptides just a gentler version of steroids? No, and that’s the exact misunderstanding this page is trying to clear up. Anabolic steroids are one defined, federally controlled class of synthetic testosterone relatives. “Peptides” covers a much wider category of short amino acid chains, from carefully trialed GLP-1 medications to barely studied research powders. They aren’t different strengths of the same thing, so calling peptides a “milder steroid” misunderstands both words.
Can either one legally be bought online without a prescription? Anabolic steroids cannot be legally obtained without a prescription under any circumstance, since they’re Schedule III controlled substances, and a “research use only” label doesn’t change that [1]. Some peptides are legitimate prescription medicines a clinician can prescribe and a pharmacy can fill, while research-status peptides sold as powders online sit in a gray market with no clinician and no pharmacy involved. Legality comes down entirely to the specific compound and the path it took to reach you.
Do GLP-1 peptides and steroids affect body composition the same way? Both can change how a body looks, but through very different mechanisms, evidence, and oversight. GLP-1 peptides like semaglutide and tirzepatide raise insulin secretion, lower glucagon, slow gastric emptying, and increase satiety, backed by a large published trial record [4][5]. Steroids build muscle by binding androgen receptors throughout the body, an effect that comes with documented cardiac and hormonal costs [2][3]. Similar goal, very different risk.
Which is safer, peptides or steroids? It depends entirely on the specific thing in question, which is why the broad version of this question doesn’t really work. An FDA-approved peptide under medical supervision is not the same proposition as an unverified research powder, and neither is the same as an illicit steroid. The comparison that actually means something is unsupervised illicit steroid use against a specific peptide obtained through medical care, and there the supervised route is clearly the more responsible one. Neither kind of compound is safe unsupervised.
Are “research use only” peptides safe simply because they aren’t controlled substances? Not being scheduled isn’t the same as being proven safe. Research-status peptides like BPC-157 and TB-500 carry limited human evidence, and a “research use only” disclaimer specifically means no clinician evaluated you and no pharmacy was involved. The lack of a federal schedule reflects how new and understudied these compounds are, not a clean bill of health.
What does the supervised path actually involve? A licensed clinician reviews your history, a prescription gets written where appropriate, a licensed pharmacy dispenses it, and someone stays medically responsible afterward. That’s the oversight layer a gray-market powder sale simply cannot offer. Supervised telehealth providers built this way, FormBlends among them, sit in a different category from a disclaimer-shipped powder, though many compounded medications in this space remain non-FDA-approved and unevaluated by the FDA for safety, effectiveness, or quality, so supervision adds oversight rather than a guarantee of equivalence to an approved brand drug.
What are peptides and steroids, really, and why do people compare them at all?
Peptides are short chains of amino acids, the same building blocks the body already uses to make proteins. Steroids are fat-soluble molecules built on a cholesterol backbone, including hormones like testosterone and cortisol. People compare them because both get used, legally and illegally, to change body composition or aid recovery. The comparison usually reflects marketing more than biology, since the two work through entirely different pathways.
Are these legitimate medical treatments, or mostly a gray-market thing?
Both categories hold fully legitimate, FDA-approved medicines alongside a sprawling gray market, so it comes down to the specific compound and where it came from. Insulin is a peptide. Prednisone is a steroid. Both are prescribed daily in clinics everywhere. The risk in either category spikes once sourcing skips a licensed prescriber, because purity, dosing accuracy, and monitoring disappear along with the prescription.
What do these therapies typically cost?
Costs swing widely depending on the compound, the dose, and whether a prescription is involved. Generic testosterone cypionate can run under fifty dollars a month through insurance. Certain peptide protocols prescribed through a physician-supervised compounding pharmacy, such as FormBlends, can run one hundred to several hundred dollars a month out of pocket. Research-chemical versions sold online may look cheaper up front but carry unknown purity risks that can cost far more down the line.
Which is better for muscle recovery?
There’s no single answer, because recovery isn’t one biological event. Anabolic steroids have the longer, better-documented track record for muscle protein synthesis, alongside meaningful side-effect profiles. Certain peptides, growth-hormone secretagogues in particular, show early promise for tissue repair and sleep, but the clinical evidence is thinner and long-term safety data is still catching up. The honest answer rests on a person’s health profile, their goals, and what a qualified clinician judges appropriate for them.
References
- Anabolic steroids are classified as Schedule III controlled substances, the same tier as testosterone and ketamine, reflecting intermediate abuse potential. Drug Scheduling, StatPearls, NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK557426/
- Systematic review and meta-analysis (35 studies, ~2,000 men): AAS associated with reduced LV ejection fraction and global longitudinal strain, increased wall thickness and LV mass. International Journal of Cardiology, 2026. https://pubmed.ncbi.nlm.nih.gov/40945618/
- AAS-related cardiovascular consequences, including hypertension, lipid disorders, cardiomyopathy, atherosclerosis, and greater coronary plaque volume vs non-users. International Journal of Molecular Sciences, 2025.
- Recovery from anabolic steroid-induced hypogonadism is variable and depends on age and degree of abuse; testosterone, testicular size, and spermatogenesis recover over months to years if at all. Endocrine Connections, 2023.
- GLP-1 receptor agonists (e.g., semaglutide) are incretin-based peptide agents that increase insulin secretion, suppress glucagon, delay gastric emptying, and increase satiety. Glucagon-Like Peptide-1 Receptor Agonists, StatPearls, NCBI Bookshelf.
- SURMOUNT-1 tirzepatide trial: mean weight loss of 15.0% to 20.9% across doses vs 3.1% placebo at 72 weeks. New England Journal of Medicine, 2022 (Jastreboff et al.).
It does not diagnose, treat, or prescribe, and it is not a substitute for a licensed clinician. Some medications described here are available only by prescription, and many are compounded preparations that are not FDA-approved and have not been evaluated by the FDA for safety, effectiveness, or quality. Talk to a licensed clinician before starting any of this. Nothing here is guidance on obtaining anabolic steroids, which are controlled substances.
Written by Zane Eriksen, science writer. Last reviewed March 2026.
Not a treatment plan. A licensed clinician should weigh in before you make any changes.